![The *intentional* [political conflating] of "Myalgic Encephalomyelitis (M.E.) (aka Enteroviral Encephalomyelitis) with "FATIGUE STATE" criterias on Australian TV (featuring Jodi Bassett of Hummingbirds' Foundation for M.E.)](https://1a-1791.com/video/s8/6/L/k/4/H/Lk4Ht.oq1b.jpg)


Dr. Nancy Klimas makes a *false equivalence* claim between Epidemic M.E. (aka Enteroviral Encephalomyelitis) & CFS "Fatigue State" criterias. She receives angry emails from Europe because she is so clearly WRONG! (A.I. Remastered Sound)
Atypical Poliomyelitis (M.E.)
Epidemic Myalgic Encephalomyelopathy
https://medical-dictionary.thefreedictionary.com/epidemic+myalgic+encephalomyelopathy
a disease superficially resembling poliomyelitis, characterized by diffuse involvement of the nervous system associated with myalgia.
Myalgic Encephalomyelitis (M.E.)
https://www.thefreedictionary.com/myalgic+encephalomyelitis
A condition of fatigue, malaise, and stress. It's cause is an "enteroviral infection" but it may be associated with recent "lung or stomach infection"
Myalgic Encephalomyelitis (M.E.), a chronic disease causing "muscle weakness and cognitive dysfunction".
Myalgic Encephalomyelitis (M.E.), identified as a new clinical entity with distinctive features in 1956, was originally considered as a neuromuscular disease.
In 1988 the Centers for Disease Control and Prevention introduced the ill-defined concept of Chronic Fatigue Syndrome (CFS). As predicted, CFS, unjustly considered to be a synonym for M.E., pushed M.E. to the background.
To develop effective therapies for of M.E. and CFS, it is essential to investigate patients with M.E. specifically.
For that reason, an operational definition of M.E. is indispensable.
This article proposes an operational definition based on the most recent formal definitions and symptoms observed in M.E.
This article proposes an operational definition based on the most recent formal definitions and symptoms observed in M.E.
M.E. is a multi-systemic illness, which
(1) often has a sudden onset, in most cases a respiratory and/or gastro-intestinal infection
(2) has an epidemic and an endemic form;
(3) has an unique clinical pattern deviating from other post-viral states;
(4) is distinguished by muscle fatigability/prolonged muscle weakness after trivial exertion;
(5) is accompanied by symptoms relating to neurological disturbance, especially of cognitive, autonomic, and sensory functions;
(6) can be accompanied by symptoms associated with cardiac and other systems;
(7) is characterized by fluctuation of symptoms (within and between "episodes");
(8) has a prolonged relapsing course; and
(9) has a tendency to become chronic.
In conclusion, a discriminative definition for M.E. contains four mandatory elements:
(1) muscle fatigability/post-exertional muscle weakness lasting for days;
(2) operational criteria for "neurological disturbance, especially of cognitive, autonomic and sensory functions";
(3) fluctuation of symptoms; and
(4) a prolonged relapsing course.
This tentative definition of M.E. justifies the qualification "neuromuscular disease".


Ampligen being blocked from release by the psychologizers
Atypical Poliomyelitis (M.E.)
https://me-pedia.org/wiki/Ampligen


Dr. Lucinda Bateman runs through the history of Epidemic M.E. (aka Enteroviral Encephalomyelitis) & invention of CFS "fatigue state" criterias.
Atypical Poliomyelitis (M.E.)
"Comparable illnesses although had been documented for centuries it's very difficult to make historical comparisons just because of the rate of change in medicine" - Dr. Lucinda Bateman
Doctor Narcissism, Arrogance, included is a Bullshit-Nonsense Excuse for Ignorance etc..
2
comments

Why do most doctors prefer "Chronic Fatigue Syndrome (CFS)" to "Myalgic Encephalomyelitis (M.E.)" ? - Dr. Charles Shepherd
Atypical Poliomyelitis (M.E.)
They have been directed to act this way as per governmental policy. They are also narcissistic gaslighters, con-artists, medically ignorant in cases and in many others 'sadistically malignant' towards patients. The institution of medicine is rotten and corrupt. OCPD-Cookbook medicine and not personalized medicine directed towards those with lived experience and personalized to the individuals, it treats or doesn't and withholds in favour of a much cheaper 'psychological perspective' and 'explanation' in regards to Myalgic Encephalomyelitis (M.E.).
It is obvious 'the medical profession' must know 'Post-Infectious Encephalomyelitis' exists but doesn't know what it is (a vasculitis of brain and spinal cord) nor how to diagnose and treat it; so acts like it doesn't exist and 'gaslights' those, who may be afflicted by such a medical disease.
Post-infectious encephalomyelitis: some aetiological mechanisms (1978) - Peter Behan
https://academic.oup.com/pmj/article/54/637/755/7063782
The possibility that acute disseminated encephalomyelitis (ADEM) and epidemic myalgic encephalomyelitis (‘epidemic neuromyasthenia’) may share a common pathogenesis is examined and many factors common to the two diseases are described. It is suggested that further study of ADEM may help our understanding of epidemic myalgic encephalomyelitis.
Dr. Charles Shepherd implies it's down to the patients to convince 'the medical establishment' and 'doctors' of their own damn disease. This is a false proposition.
The medical professional are wholely and solely at fault and to blame for the mistreatment of patients with Myalgic Encephalomyelitis (M.E.).
They are negligent, incompetent, gullible, conditioned and bureaucratically controlled and have to adhere to cost effectiveness even if it's harmful towards patients. DO NO HARM is completely ignored in the case of Myalgic Encephalomyelitis (M.E.) patients. It's deemed cheaper and more cost effective to psychologize chronic infection, encephalitic or encephalomyelitic brain injuries and resulting disabilities on purpose and to adhere to government policy. Government, Doctors, Hospitals, Nurses, Psychiatry, Psychiatric Hospitals and even charities placed to protect patients, lead abuse of patients.
What is worse, there is no excuse for any of it or for the ability of Myalgic Encephalomyelitis (M.E.) to be recognized ?
ENCEPHALOMYELITIS RESEMBLING BENIGN MYALGIC ENCEPHALOMYELITIS (1970) - Innes
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(70)91097-4/fulltext
Four cases of 'Encephalomyelitis resembling benign Myalgic Encephalomyelitis' are reported. A Coxsackie B2 virus was isolated from the cerebrospinal fluid in one case and an echovirus type 3 virus from the fæces and the cerebrospinal fluid in another. Serological tests indicated Coxsackie B2 and Coxsackie B5 infection in the other two cases.
Myalgic Encephalomyelitis--a persistent Enteroviral infection? (1990)
https://academic.oup.com/pmj/article/66/777/526/7061518
Myalgic Encephalomyelitis is a common disability but frequently misinterpreted. Amongst 6,000 patients referred for general microbiological diagnosis between 1975 and 1987, 420 cases were recognized. Coxsackie B neutralization tests, in 205 of these, demonstrated significant titres in 103/205 (50%), while of 124 additionally investigated for enteroviral IgM, 38/124 (31%) were positive. This illness is distinguished from a variety of other post-viral states by an unique clinical and epidemiological pattern characteristic of 'Enteroviral' infection. Prompt recognition and advice to avoid over-exertion is mandatory. Routine diagnosis, specific therapy and prevention, await further technical advances.
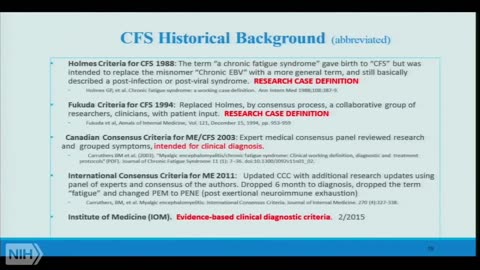
Myalgic Encephalomyelitis (M.E.) or What? An Operational Definition (2018)
https://www.mdpi.com/2075-4418/8/3/64
Myalgic Encephalomyelitis (M.E.), identified as a new clinical entity with distinctive features in 1956, was originally considered as a Neuromuscular Disease. In 1988 the Centers for Disease Control and Prevention introduced the ill-defined concept of Chronic Fatigue Syndrome (CFS). As predicted, CFS, unjustly considered to be a synonym for M.E., pushed M.E. to the background. To develop effective therapies for of M.E. and CFS, it is essential to investigate patients with M.E. specifically. For that reason, an operational definition of M.E. is indispensable. This article proposes an operational definition based on the most recent formal definitions and symptoms observed in M.E.
Nightingale Research Foundation Definition (2016)
https://me-pedia.org/wiki/Nightingale_Research_Foundation_definition
The Nightingale Research Foundation definition is a definition of Myalgic Encephalomyelitis (M.E.) that was developed by the Nightingale Research Foundation. It was first presented as a preliminary draft in 2006, published in 2007, and updated in 2016.
International Consensus Criteria (ICC) (2011)
https://www.me-pedia.org/wiki/International_Consensus_Criteria
International Consensus Criteria (ICC) is a medical consensus criteria that can be associated with Myalgic Encephalomyelitis (M.E.), is a chronic, inflammatory, physically and neurologically disabling disease. For pediatric and adult cases a diagnosis should be made immediately; there is no need to wait up to 6 months.
Medical Narcissism
https://en.m.wikipedia.org/wiki/Medical_narcissism
Medical narcissism is a term coined by John Banja in his book, Medical Errors and Medical Narcissism.
Banja defines "medical narcissism" as the need of health professionals to preserve their self-esteem leading to the compromise of error disclosure to patients.
In the book he explores the psychological, ethical and legal effects of medical errors and the extent to which a need to constantly assert their competence can cause otherwise capable, and even exceptional, professionals to fall into narcissistic traps.
Q: You are saying that it is uncertain as to whether there is an actual inflammation within the brain and the spinal cord. I think most (99,9 %) of the patients didn't get any testing for that. So how can you say there is no inflammation of the brain? I myself feel it every day.
A: I am one of the few doctors who is involved in post-mortem research, and the results from a small number of these post-mortems have been published. The bottom line here is that encephalitis (widespread inflammation in the brain) has not yet been found in these PMs. Neither has widespread inflammation in the spinal cord been found. What we have found is dorsal root ganglionitis - inflammation of tiny nervous structures that lie just outside the spinal cord in the peripheral nervous system and are responsible for processing sensory information like pain and touch.
Q: It can't be found on scans?
A: You can make a diagnosis of an acute encephalomyelitis through a combination of clinical history, examination findings and abnormalities on neurological investigations, including scans. But you do not see this combination in people with "ME/CFS"
(There is "no such thing" as "ME/CFS" it's the medical conflation of "Enteroviral Encephalomyelitis" with numerous "FATIGUE STATE" criterias, in which it's excluded from by the very nature of the neurological disease)
Q: How can the large differences between patients be explained? Why are some patients
bedridden, while others still are able to work and have some social life?
A: Nobody has a satisfactory answer as to why some people with "ME/CFS" improve, others remain more static and variable, whereas others become severely affected. Partly because so little research has been done on people with "Severe M.E."
The MEA has funded research into factors that may be involved in "severe M.E." and the M.E. (blood sample) Biobank at UCL in London that we are funding is collecting blood samples from people with "severe M.E." to see if there are any characteristic differences in severe cases.
Q: You said you catched M.E. (he didn't because he developed Herpes Zoster Encephalitis and not M.E.) from a patient. Is M.E. contagious?
A: I caught "chickenpox virus" from a patient of mine who had shingles (same virus). The CP virus, then triggered my "M.E." (Dr. Charles Shepherd didn't develop M.E. but a disability caused by Herpes Zoster Encephalitis, which is NOT Royal Free Disease). It is the triggering infection that can be spread to other people. There is no evidence that "ME/CFS" (there is no evidence that a disease named "ME/CFS" even exists and is an oxymoron) can be passed from person to person.
Q: So you mean that M.E. is the outcome of a disease instead of a disease itself. It can have
numerous causes? (it is a specific disease, it's self, no there is NOT different causes)
A: A large number of viral infections, including hepatitis, can trigger "ME/CFS" (aka "misdiagnosed" CFS illnesses). It can also be
occasionally triggered by non viral infections (e.g. salmonella) and other types of immune
system stressors such as vaccinations. I have a large collection of people with "ME/CFS" who predate the onset to a vaccination - health workers following hepatitis B vaccine in particular
Q: And is the trigger that causes the M.E. responsible; if you get "mild" (there is no such thing as mild M.E.) or "severe M.E." ?
A: Think of "ME/CFS" (it does not exist as a specific medical disease, it is a FATIGUE STATE criteria) as a three stage process involving 3Ps. Genetic factors that Predispose to its development. Immune system stressors (e.g. infections) that Precipitate the illness, And a complex range of resulting abnormalities involving brain, immune system, endocrine system that Perpetuate the illness
Q: Are there perspectives in the development of a medicine or are the researchers groping
entirely in the dark where the disease is lodged in the body?
A: ME/CFS (it's a FATIGUE CRITERIA not a specific medical disease) is perpetuated by a complex interaction between abnormalities involving brain, muscle, endocrine/hormone system and immune systems. Until we understand more about these abnormalities and how they interact it is going to be difficult to find a drug treatment that deals with the underlying disease process.
One promising lead which you may have heard about is a drug called "Rituximab" (totally inappropriate for anybody chronically infected with an "enterovirus", so not appropriate for M.E.). This is normally used to treat people with lymphoma - a type of cancer. But some Norwegian doctors have found that it appears to benefit a subgroup of people with ME/CFS (aka a CFS illness). The reason for this may be due to the fact that "Rituximab" dampens down a part of the immune system that produces autoantibodies - harmful antibodies that can attack/damage healthy tissues and organs.
Q: You are saying in your video using ‘opathy’ takes the "heat" out the situation - of course it does, for it still leaves the diagnosis wide open to how you want to choose to interpret it : mental or physical. Because the word ‘opathy’ , exactly like "CFS", has a dual interpretation : it can be interpreted physically and/or psychiatrically. So how do you make clear, which one is which?
A: I obviously have considerable sympathy with people who believe this illness should be
called "Myalgic Encephalomyelitis (M.E.)" as my own illness was triggered by a "Chickenpox Encephalitis" (clearly not "Enteroviral Encephalomyelitis" then; so not "Epidemic" Myalgic Encephalomyelitis (M.E.) so Charles Shepherd is "NOT" an M.E. Sufferer)
But in our current state of knowledge I do not believe that M. encephalomyelitis is a correct
way of describing the pathology. This is why I have advocated the use of the term M.
encephalopathy - as this is consistent with the abnormalities that have been published
Q: In your talk of 25 February (36), you proposed a new name instead of M.E. or CFS: Myalgic Encephalopathy, in order to reduce the confusion about the name. But, given the fact there is a lot of research, would it not be wise to wait with a new name until the "final" cause(s) of this illness have been found? A third name can even increase the confusion.
Q: Dr. Shepherd, in the interview you state that there are no confirmative tests for M.E.. Others maintain that they have such tests (e.g. Byron Hyde MD, John Chia MD).
Why, do you think, is there such a difference of opinion among experts?
A: I wish we had a biomarker or test (blood, neuroimaging etc... ) that could confirm that
someone has "ME/CFS" (Obviously there is no such medical disease as "ME/CFS") but that is just not the case at present. I know that some of my colleagues believe that they have such tests - but this view is not shared by the majority of docs working in this area.
(So not medical Expertise medicine, Medical consensus medicine, ridiculous and insane. I am interested in who is right, not a consensus, which can be WRONG).
A: I proposed a new name - Myalgic Encephalopathy - at a time when there was
tremendous pressure on the medical establishment to get rid of "Myalgic Encephalomyelitis" here in the UK, where many doctors just will not use the term M.E. because they do not believe it reflects the pathology.
Q: Do you still support the name Myalgic Encephalopathy, or are you now convinced that M.E. involves CNS inflammation?
A: I still support and use the term Myalgic Encephalopathy in preference to Myalgic Encephalomyelitis.
Whilst I do not believe that M.E. involves widespread inflammation in the brain and spinal cord I do believe that neuroinflammation plays a role - and this is one of the MRC research priorities here in the UK. I am one of the few docs involved in post-mortem research and our group have published preliminary results supporting a role for neuroinflammation in ME/CFS- i.e. the presence of "dorsal root ganglionitis" in some cases. If you remind me on MEA Facebook later I will give you the reference.
Q: In terms of neuro research are we going to find damage or an ongoing infection do you think?
A: In relation to neuro research "I would be surprised if we find evidence of on-going infection" or "significant structural damage". If this was the case "I think it would have been shown by now".
What is encouraging is that new forms of neuroimaging mean that we can learn much more about brain activity, blood flow etc
And along with info on brain chemical transmitter activity this means that we could get a better understanding of the underlying disease process and effective forms of treatment"
Q: Dr. Shepherd do you agree with the majority of British doctors, NICE etc... and see M.E. as a psychiatric or psychological condition?
A: I would say that most UK doctors view M.E. or ME/CFS as a combination of physical and psychological. A minority view it as purely physical and another minority view it as purely psychological. A small number still do not believe, that they exist as clinical entities.
Political Abuse of Psychiatry
https://en.m.wikipedia.org/wiki/Political_abuse_of_psychiatry
Political abuse of psychiatry, also commonly referred to as punitive psychiatry, is the misuse of psychiatry, including diagnosis, detention, and treatment, for the purposes of obstructing the human rights of individuals and/or groups in a society. In other words, abuse of psychiatry (including that for political purposes) is the deliberate action of having citizens psychiatrically diagnosed who need neither psychiatric restraint nor psychiatric treatment. Nowadays, in many countries, political prisoners are sometimes confined and abused in psychiatric hospitals. Psychiatry possesses a built-in capacity for abuse that is greater than in other areas of medicine. The diagnosis of mental disease allows the state to hold persons against their will and insist upon therapy in their interest and in the broader interests of society. The use of hospitals instead of jails also prevents the victims from receiving legal aid before the courts in some countries, makes indefinite incarceration possible, and discredits the individuals and their ideas. The political abuse of the power entrusted to physicians, and particularly psychiatrists, has a long and abundant history, for example during the Nazi era and the Soviet rule when religious and political dissenters were labeled as "mentally ill" and subjected to inhumane "treatments". In the period from the 1960s up to 1986, abuse of psychiatry for political and ideological purposes was reported to be systematic in the Soviet Union, and occasional in other Eastern European countries such as Romania, Hungary, Czechoslovakia, and Yugoslavia. Political abuse of psychiatry also takes place in the People's Republic of China.
The Chronic Fatigue Syndrome (aka ME/CFS) Umbrella - Profound Fatigue, Pain, Inflammation, Poor Sleep, Exercise Intolerance & Exhaustion, Relapse after Exercise - Dr. Nancy Klimas (A.I. Remastered Sound)
Loading comments...
-
![Days Gone: Old Country Road - Part 3 [PC] | Rumble Gaming](https://1a-1791.com/video/s8/1/Q/q/G/_/QqG_u.0kob-small-Days-Gone-Old-Country-Road-.jpg) LIVE
LIVE
NeoX5
3 hours agoDays Gone: Old Country Road - Part 3 [PC] | Rumble Gaming
391 watching -
 LIVE
LIVE
CAMELOT331
2 hours agoRide N' Die 24 Hour LAUNCH Ft Ethan Van Sciver, Cecil, ItsaGundam, That Star Wars Girl, Shane & MORE
401 watching -
 12:53
12:53
DeVory Darkins
16 hours ago $4.38 earnedKamala Intoxicated Video Message to Staff Shocks Internet
8.94K38 -
 UPCOMING
UPCOMING
Mally_Mouse
3 hours agoLet's Yap About It - LIVE!
157 -
 21:59
21:59
Midnight's Edge
1 day agoElon Musk calls out Norway for destroying its own future!
4863 -
 3:23:26
3:23:26
Pardon My Take
8 hours agoSUPER MEGA THANKSGIVING PREVIEW, KIRK COUSINS WANTS TO BE IN WICKED 2 + PFT/HANK RIVARLY CONTINUES
5.04K2 -
 44:59
44:59
The Kevin Trudeau Show
3 hours agoWhat Women Do Wrong in Relationships (From a Man’s Perspective) | The Kevin Trudeau Show | Ep. 69
10.7K4 -
 19:49
19:49
This Bahamian Gyal
14 hours agoFIRED after VENTING online about ELECTION results
5.28K9 -
 LIVE
LIVE
REVRNDX
4 hours agoYOUR NEW FAVORITE RUMBLE STREAMER
105 watching -
 1:04:41
1:04:41
Russell Brand
3 hours agoIs This the End? Climate Emergencies, Kamala’s Chaos & Political Meltdowns EXPOSED! – SF502
97.1K273