The Use of Lasers in Thoracic Surgery
http://festyy.com/edDveK
The Use of Lasers in Thoracic Surgery - CHEST Journal
https://journal.chestnet.org › article › full text
by SM Shapshay · 1985 · Cited by 7 — Applications of the laser in thoracic surgery to seal lung tissue during open operation and perhaps through a thoracoscopy, approach are promising areas of ...
People also search for
The application of the laser in medicine continues to expand in various specialities including bronchology and, most recently, thoracic surgery. Endoscopic application of laser technology began in 1973 with the use of the carbon dioxide (CO2) laser to ablate benign lesions, such as tracheobronchial papilloma and, later, to palliate malignant obstruction of the airway.1, 2 However, problems associated with a somewhat cumbersome arm mirror-to-lens delivery system and the limited hemostasis associated with the CO2 laser prompted the application of the neodymium-yttrium aluminium garnet (Nd-YAG) laser in bronchology.3, 4 With its superior hemostatic qualities, the Nd-YAG laser can be delivered through a flexible quartz fibre that is easily passed through standard or somewhat modified flexible and rigid fiberoptic bronchoscope systems. Large series of patients with malignant tracheobronchial obstruction have undergone successful palliation with minimal rates of morbidity, according to reports by a number of investigators3, 5 in Europe and the United States.
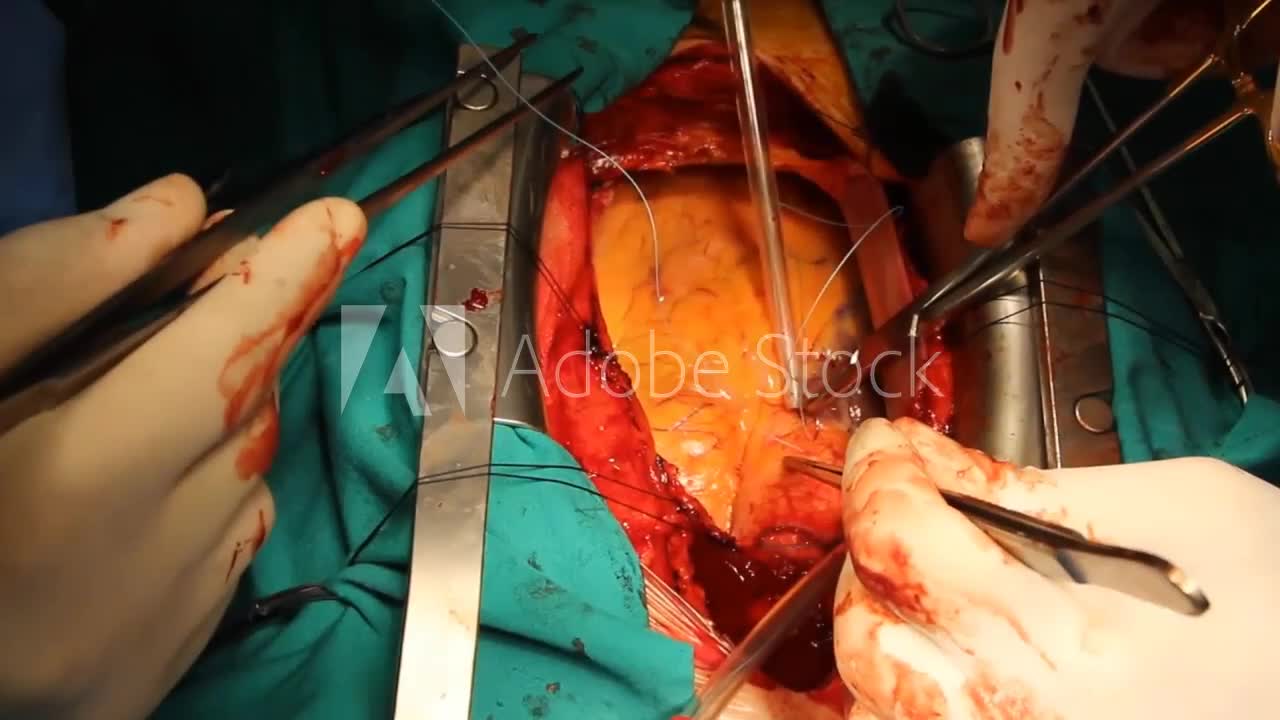
Applications of the laser in thoracic surgery to seal lung tissue during open operation and perhaps through a thoracoscopy approach are promising areas of investigation. In this issue of Chest (see page 820), LoCicero et al clearly show that, when used in a defocused manner, the CO2 laser can “weld” small (1 mm by 3 mm) holes in lung tissue with minimal pleural adhesion.
However, defects of this size are of no clinical consequence in thoracic surgery since they seal spontaneously. Laser technology would be of value in the treatment of spontaneous pneumothorax if it can be used through a thoracoscopic approach.
Open transthoracic bleb resection using staplers or sutures combined with pleurectomy or pleural abrasions is highly successful, and the use of expensive laser technology and longer hospitalization in this setting are unwarranted.
On the other hand, the authors point out three uses of the laser in pulmonary surgery that have great promise. The first of these is subsegmental resection of solitary pulmonary nodules or multiple metastatic lesions. With the use of the laser, such lesions with adequate histologic margins might possibly be removed in a cordlike fashion, without sacrificing a considerable amount of surrounding lung tissue. The second potential use is in pulmonary lobectomy when an incomplete fissure is present.
A stapling device, which is often used in such situations, may cause unnecessary distortion of the lung. Laser dissection might also be useful in segmental lung resection, a procedure often associated with prolonged leakage of air. The third potential application is thoracoscopic lung biopsy in immunocompromised patients, using the laser either to seal an area of forceps biopsy or as a cutting device to perform the biopsy.
Questions may arise, such as, “Is this the right laser?” and “How does this procedure compare with electrocautery, which is a lot less expensive?” Experimental work by Wolfe et al6 indicated that effective control of air leaks was achieved with less tissue necrosis using the Nd-YAG laser compared with electrocautery. The Nd-YAG laser is a better coagulator of tissue than the CO2 laser, perhaps providing more secure welding of the lung.
About us https://bit.ly/3GUPFOa
Contact us +919942258153 kvk.subadhra@gmail.com
https://9612d85c5805iy1pqsyboaso9z.hop.clickbank.net
-
 3:25:11
3:25:11
Akademiks
14 hours agoPRE SUPERBOWL STREAM! Will Kendrick END Drake Career Tonight? Will Drake and PND outsell DOT?
141K14 -
 DVR
DVR
Vigilant News Network
14 hours agoEfforts to BAN Dangerous COVID Jabs Underway | Media Blackout
102K44 -
 1:49:02
1:49:02
VIVA TV
3 days agoWhat Is The Most Shocking Sports Story Of The 2000's? (The Bracket, Vol. 161)
182K20 -
 3:07:41
3:07:41
TheNateVibez
16 hours ago#1 Streamer in Kentucky👀 - T-800 Road to Rank Domination✌ - ArmyVet🫡
118K2 -
 4:03:05
4:03:05
EXPBLESS
16 hours agoHAPPY FORTNITE SUB SUNDAY - SUB GOAL {8-50} #RUMBLEGAMING
97.8K2 -
 9:19
9:19
VSiNLive
1 day agoYou MUST Consider These 3-LEG PARLAYS for Super Bowl LIX!
129K6 -
 9:21:08
9:21:08
Scottish Viking Gaming
19 hours ago💚Rumble :|: Sunday Funday :|: If you can't Beat them...EAT THEM!!
112K4 -
 1:46:47
1:46:47
Game On!
1 day ago $15.75 earnedExpert Super Bowl LIX Picks, Preview, and Best Bets!
190K15 -
 36:50
36:50
Mrgunsngear
1 day ago $32.50 earnedPresident Trump's Executive Order To The ATF: This Could Be Huge!
154K87 -
 25:48
25:48
Adam Does Movies
1 day ago $4.70 earnedTop 10 Reasons Why Emilia Pérez Is Complete TRASH!
102K7